![Diseases, Symptoms, tcm, [tcmwindow.com]](/uploadFile/adImg/2015/11/11/f5cbfcc0-4df5-4646-9b9a-f316651a0199.jpg)






Over half of all women experience primary dysmenorrhea, and many consider their menstrual pain inevitable. However, the prevalence of pain implies neither normalcy nor necessity. In the occident, acupuncture has recently gained popularity for women's reproductive health conditions, especially infertility. Nevertheless, believing that pain an inevitable consequence of being born a woman, many do not seek acupuncture to treat their dysmenorrhea; in some cases, it is only after seeking out acupuncture for other conditions that women are educated in its potential to treat their menstrual pain. In Traditional Chinese Medicine (TCM), dysmenorrhea (including menstrual pain and other pre-menstrual symptoms) is considered a disorder just as worthy of treatment as any disease. Researchers at The National Institute of Complementary Medicine at Western Sydney University in Australia conducted a study to compare the efficacy of manual acupuncture and electro-acupuncture, at two timing intervals, for the treatment of primary dysmenorrhea. The researchers found that, in all cases, acupuncture leads to a significant reduction in the intensity and duration of menstrual pain after three months of treatment, and the results were sustained one year after trial entry. This study, along with others in the same vein, will hopefully be encouraging for those women who suffer each month from dysmenorrhea.
Primary dysmenorrhea is menstrual pain that has no identified organic cause; women with endometriosis, or other biomedically defined uterine conditions, may have menstrual pain, but that pain is considered secondary dysmenorrhea since the etiology is known. Primary dysmenorrhea is most common in young women under the age of 25. The characteristic symptoms are cramps - colicky spasms of pain in the suprapubic area - occurring within 8–72 hours of menstruation, and the pain usually peaks with the increase in menstrual flow during the first few days of a woman's menstrual cycle. "In addition to painful cramps, many women with primary dysmenorrhea experience other menstrual-related symptoms, including back and thigh pain, headaches, diarrhoea, nausea and vomiting." Iacovides et al. note that "the prevalence of primary dysmenorrhea is highly underestimated, yet difficult to determine, because few affected women seek medical treatment, despite the substantial distress experienced, as many consider the pain to be a normal part of the menstrual cycle rather than a disorder…. Prevalence estimates vary between 45 and 95% of menstruating women, with very severe primary dysmenorrhea estimated to affect 10–25% of women of reproductive age. As such, dysmenorrhea appears to be the most common gynecological disorder in women irrespective of nationality and age.
Amongst women, dysmenorrhea is the most common cause of absenteeism from school and work, and it may also lead to "a reduction in academic performance, reduced participation in sport and social activities and an overall significant decrease in women's quality of life. Despite the significant negative impact and disruption to daily living that primary dysmenorrhea has on women most do not seek medical treatment. When women do present to their doctor with primary dysmenorrhea, the most commonly prescribed treatments are non-steroidal anti-inflammatories (NSAIDs) and the combined oral contraceptive (COC) pill." While these treatments help some women, they are ineffective or unpalatable for others. "Lack of satisfaction in standard treatment leads to an increase in self-care, with women commonly using complementary therapies to deal with their menstrual pain in addition to, or instead of, pharmaceutical pain relief, due to a lack of perceived effectiveness or a dislike of using analgesic medication" Alternative therapies such as acupuncture are gaining traction as women find practitioners that take their conditions seriously and offer tangible relief without medication.
In Traditional Chinese Medicine (TCM), dysmenorrhea refers to recurrent abdominal or lumbosacral pain experienced before, during, or after menstruation. According to TCM theory, there are three primary etiologies, each manifesting according to its root cause: liver qi stagnation, cold accumulation, and qi and blood deficiency. Liver qi stagnation causes distending pain in the lower abdomen, which may refer to the waist and back; when qi stagnation leads to blood stasis, there may be spells of sharp, stabbing pain, which is relieved by the passing of small clots of menstrual blood. Stagnated liver qi can also cause the irritability and emotional issues associated with PMS. Similarly, cold accumulation will slow and coagulate the blood, causing blood stasis; this pattern causes the sharp, stabbing pain associated with blood stasis, as well as the cramping or contracting of the uterine muscles due to cold accumulation. Alternatively, deficient qi and blood fail to nourish the uterus, leading to dull, aching pain that may occur during or after menstruation. Both the excess cold and qi and blood deficiency patterns can be alleviated by warmth, and thus moxibustion - the burning of mugwort on or near the body at acupoints or around the area of pain - is indicated for both of these etiologies. According to Hsu et al., "the syndrome of cold coagulation and blood stasis is mostly seen," though, considering how few women seek out treatment for dysmenorrhea, it is possible that this pattern is more common clinically because of the extreme pain and cramping associated with this pattern, as compared to the relatively mild - or manageable - pain associated with the patterns.
According to scientific studies, dysmenorrhea is linked to an increase in both the tension and contraction frequency of the uterine muscles, as well as a discord in the rhythm of shrinkage; the uterine muscles contract and do not relax fully between contractions. These abnormalities cause a disorder in uterine micro-circulation that leads to ischemia and hypoxia. Tests conducted on lab rats by Hsu et al. find, "dysmenorrhea of the cold coagulation syndrome presents a high intensity of uterine tension and high contraction of the microvascular diameter, the uterine microcirculation, and tension have negative correlation. The uterine microvascular and capillary contraction decreases the uterine microvascular blood flow and increases uterine contraction wave number. This furthermore explains that dysmenorrhea could cause uterine muscle spasm, increase contraction, and produce microcirculation disorder. Accordingly, it proves that uterine contraction and uterus microcirculation are closely related to dysmenorrhea environment."
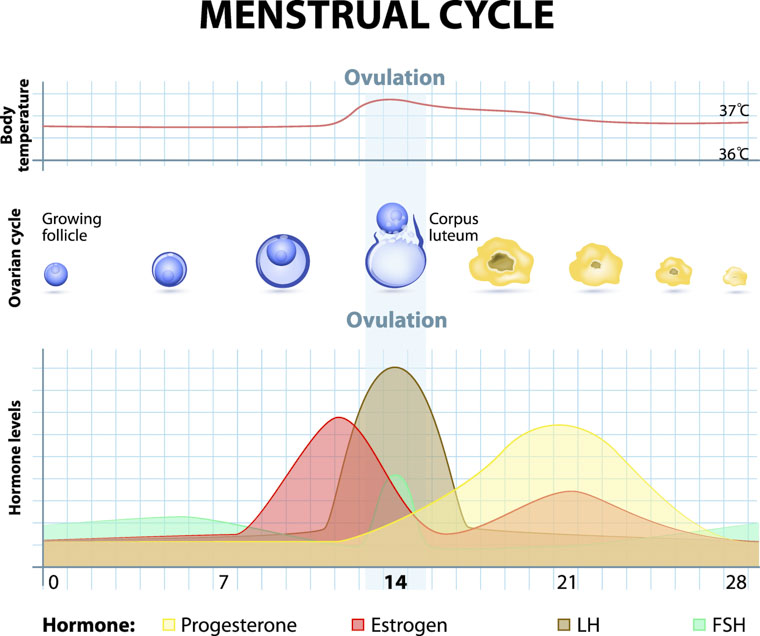
The prevailing theory is that the changes in uterine micro-circulation and contractility associated with dysmenorrhea are related to the disordered production of endometrial prostaglandins (PGs), endogenous hormone-like lipid compounds. During the luteal phase, women have increased levels of PGs. However, women with dysmenorrhea have notably higher levels of circulating PGs than eumenorrheic women, especially during the first 48 hours of their menses, when their symptoms peak. Furthermore, "the severity of menstrual pain and associated symptoms of dysmenorrhea are directly proportional to the amount of PGs released," confirming that altered PG levels are the likely cause of pain. In another study, Zahradnik et al. studied the menstrual blood collected from both eumenorrheic and dysmenorrheic women and found that dysmenorrheic women had a concentration of prostaglandin F2α (PGF2α) that was 2.5 times higher than eumenorrheic women, though their levels of prostaglandin E2 (PGE2) were identical. [12] Hsu et al. attributed dysmenorrheic pain to this increase in the ratio between PGF2 and PGE2: "while PGE2 may result in either myometrial contraction or relaxation, PGF2a always causes potent vasoconstriction of uterine blood vessels, and myometrial contractions." As vasoconstriction causes a decrease in blood flow, myometrial contractions increase the need for oxygenated blood; the prevalence of these two factors together lead to hypoxia. Doppler ultrasonography, used to investigate uterine blood flow, has similarly shown, "that the strong and abnormal uterine contractions in women with dysmenorrhea during menstruation are associated with reduced uterine blood flow and resultant myometrial ischemia, and hence pain." [14] PGs also have a range of biological effects on a wide variety of physiological and pathological activities - including pain, inflammation, body temperature, and sleep regulation- so disproportionate production may be related to some of the secondary effects of dysmenorrhea as well.
There are a variety of theories regarding the mechanisms by which TCM therapies can relieve pain from dysmenorrhea. Armour et al. suggest there are "plausible mechanisms of action for acupuncture to improve primary dysmenorrhea, including endogenous opioid release, reduction of inflammation, alterations in uterine blood flow and changes in prostaglandin levels." In a study conducted by Yang et al. to investigate the efficacy of moxibustion at the acupoints CV4 (Guanyuan), CV8 (Shenque), and SP6 (Sanyinjiao), the researchers found that pain levels decreased over the three month trial, and that the therapeutic effect of moxibustion was sustained in the three months after the trial ended. Through blood tests, the researchers also found that moxibustion decreased levels of both PGF2 and PGE2, which allows for increased blood flow and decreased contractility of the uterus. Heat is also well understood to regulate menstrual pain - "an abdominal heat wrap was found to be as effective as ibuprofen, and more effective than acetaminophen in relieving dysmenorrheic pain" - and thus it is not surprising that heat from moxa, especially directly over the abdomen, would be similarly effective for inducing vessel dilation and increasing blood flow to decrease pain. The acupoint SP6 (Sanyinjiao) may be distal, but it is effective for the treatment of dysmenorrhea, "likely due to the fact that SP6 is segmental to the uterus… This segmental activation at the level of sacral spinal nerve 2 (S2) may lead to reflex sympathetic inhibition of the uterus resulting in increased uterine blood flow."
In the exploratory study conducted by Armour et al., the researchers used a 2x2 factorial design "to test the individual and combined effects of changing 1) treatment timing, and 2) mode of stimulation. This study used a pragmatic clinical trial design with some qualifications, including the use of a manualised acupuncture protocol designed to reduce the amount of variation between practitioners." Each patient was given acupuncture by one of two modalities: manual acupuncture (MA) or electro-acupuncture (EA). Manual acupuncture is the insertion of fine needles at specific points on the body which, in this trial, were stimulated again 10–15 minutes after insertion; electro-acupuncture uses the same points but adds electrical stimulation to the points. In this case, an ITO ES-160 electro-acupuncture machine with a 2Hz / 100Hz square wave pulse of 200ms for 20 minutes was employed.
DeQi was obtained at all acupoints at the beginning of the treatment. "DeQi (the arrival of Qi) is the sensation generated by the insertion and/or manipulation of an acupuncture needle in an acupuncture point," and TCM practitioners consider this important an important variable in the efficacy of a treatment. For the patient, DeQi feels like soreness, pressure, or heaviness at the site of insertion; for the practitioner, it is an indication that the qi has begun to flow at the acupoint, accessing the unique energy of the point to heal.
Treatment timing was tested by separating the participants into high and low frequency test groups. "All women in the study were scheduled to receive 12 treatments over the course of three menstrual cycles. Women in the high frequency (HF) group received three treatments in the seven days prior to the estimated day one of the menstrual cycle. Women in the low frequency (LF) group received three treatments in the time between menses, approximately every seven to ten days' dependent on cycle length." The 2x2 factorial design lead to a total of 4 test groups: LF-MA, HF-MA, LF-EA, and HF-EA.
Treatment was based on the eight principles of TCM, as well as Zang Fu (visceral organ) diagnosis. "Once a TCM diagnosis had been ascertained, the practitioners had the flexibility with their point selection to address the diagnosed pattern of disharmony as per the treatment handbook." Up to two concurrent patterns of disharmony were supported by this trial, distinguished into primary (root) and secondary (branch) patterns. No more than 7 unique acupoints were chosen for each patient, according to the diagnosis, and all points were needled bilaterally, with the exception of those for which unilateral insertion is indicated, such as opening the extraordinary vessels. "Each pattern also has moxibustion as a compulsory, optional or forbidden component of the treatment. Indirect moxa was administered via smokeless moxa stick for 5–10 minutes on one of the selected acupuncture points. Each patient was given a diet and lifestyle advice sheet during their first treatment session. These were grounded in TCM theory."
The primary outcome of this study was the decrease in peak menstrual pain one year after trial entry. All groups showed a significant reduction in peak pain and duration of pain over time, and neither the mode nor frequency of treatment showed a stronger effect by the one-year follow-up. However, manual acupuncture provided more immediate pain reduction. "The proportion of responders with clinically significant pain reduction of 30% in their peak pain was highest in the HF-MA group across all three days (55%, 60% and 61% of women respectively) and over a third of women in this group had a 70% reduction in their peak pain. Almost three-quarters (72%) of the women in the HF-MA group had a clinically significant 30% reduction in their average pain, with 69% of the LF-MA group, 61% of the LF-EA group and the 47% of the HF-EA group achieving this reduction. Almost 60% of the LF-MA group and 55% of the HF-MA group had a 50% reduction in average pain from baseline to one-month follow-up. The electro-acupuncture groups had lower scores, with 42% and 33% of the HF-EA and LF-EA groups achieving a 50% reduction."
The researchers also compared health related quality of life (HRQoL), supplementary analgesic use, and secondary symptoms. HRQoL measures subjective physical and mental well-being, by collecting participant data on factors including body pain, vitality, social function, and mental health. Decreased nonsteroidal anti-inflammatory drug (NSAID) use, measured in mean doses per day, is thought to be another way of measuring pain relief, since patients will only take medications once their pain meets their personal threshold. Secondary symptoms may vary between women, but common symptoms include mood changes, bloating, and breast tenderness. The results indicate that high frequency and manual treatments show better results for these factors. "Health related quality of life increased significantly in six domains in groups having high frequency of treatment compared to two domains in low frequency groups. Manual acupuncture groups required less analgesic medication than electro-acupuncture groups." More specifically, manual acupuncture provides the same - or greater - pain relief, while simultaneously decreasing the analgesic medication required. Of all groups, HF-MA had the best results for the reduction of secondary menstrual symptoms compared: "after the course of acupuncture treatment, participants had less problems with work or daily activities as a result of their physical health, less pain and subsequent limitations due to pain, more energy, and less interference from physical and emotional problems in social activities, all of which are commonly experienced by women with primary dysmenorrhea." The use of moxa for indicated conditions, which was found by Yang et al. to regulate PGF2 and PGE2 levels, [37] may have also contributed to the lasting effects of the course of treatment.
While this study did not include a control group that did not receive acupuncture treatment, a previous study conducted by Armour "that included a no-treatment or wait-list control group showed that the acupuncture intervention appeared to provide an immediate analgesic effect, irrespective of the dose delivered," and that treatment before the onset of menses produced greater pain reductions than treatment during menstruation. Other studies focus on point selection and technique. Zhao et al. found that SP6 (Sanyinjiao) is the most commonly used acupoint to treat dysmenorrhea, inducing significant analgesic effects, and that achieving DeQi, "improves the immediate analgesic effect of acupuncture at SP6 in patients with primary dysmenorrhea," especially for those patients with the specific TCM diagnosis of cold and dampness stagnation. Hsu et al. found similar results in rats, showing that acupuncture at SP6 with DeQi significantly increased microvascular uterine blood velocity as compared with the model control group that received the same treatment without DeQi.
Self-care advice may also play an important role in TCM treatment. Both practitioners and their patients have expressed that acupuncture treatment is "more than needles," and women interviewed about their experience with acupuncture for the treatment of dysmenorrhea felt that, "TCM self-care advice was related to positive outcomes for their dysmenorrhea and increased their feelings of control over their menstrual symptoms." Women responded well to the advice regarding diet and lifestyle choices and, "discussed how the context in which these explanations and advice were delivered, in a nonjudgmental and supportive environment, was different to their previous experiences with general practitioners and how this relationship with their acupuncture practitioners impacted their ability to understand their menstrual cycle better and implement the self-care advice given." Additionally, TCM practitioners tend to spend more time talking - and most importantly, listening - to their patients, allowing practitioners to better understand the life-world of the client and provide explanations and self-care advice that was appropriate and achievable for the individual, whereas patients often report that they do not get sufficient explanations for their condition from orthodox medical consultations. Furthermore, "empathy from practitioners has been shown to increase enablement and is linked to positive treatment outcomes through the improvement of self-efficacy. Improved self-efficacy is also linked to increased optimism of future improvements." The women interviewed overwhelmingly confirmed that the explanations about menstrual physiology, as well as the advice on self-care, increased their self-efficacy.
The most important result of this study, and others like it, is that menstrual pain is not inevitable. Many women may feel that medications - either NSAIDs or oral contraceptives - are their only option for treating their monthly symptoms, but acupuncture has been shown to be equally effective, and its effects last long after the course of treatment. Additionally, TCM practitioners provide individualized advice that helps women take an active role in caring for themselves. Acupuncture can provide a safe and effective alternative to medications. This study shows that the abdominal pain and emotional symptoms of primary dysmenorrhea can be addressed with TCM, and it will hopefully empower women to address their menstrual pain holistically and efficiently.
Notes:
1 Armour, Mike, Hannah G. Dahlen, Xiaoshu Zhu, Cindy Farquhar, and Caroline A. Smith. "The role of treatment timing and mode of stimulation in the treatment of primary dysmenorrhea with acupuncture: An exploratory randomised controlled trial." Plos One 12, no. 7 (2017). pg 2.
2 Armour et al, The role of treatment timing and mode of stimulation, pg 2.
3 Iacovides, Stella, Ingrid Avidon, and Fiona C. Baker. "What we know about primary dysmenorrhea today: a critical review." Human Reproduction Update vol 21, no 6, (2015). Pg 764.
4 Armour et al, The role of treatment timing and mode of stimulation, pg 2.
5 Armour et al, The role of treatment timing and mode of stimulation, pg 2.
6 Cheng, Xinnong, ed. Chinese Acupuncture and Moxibustion. Beijing: Foreign Languages Pr, 2012. Pgs 475-477.
8 Hsu, Wing-Sze, Xiao-Yu Shen, Jia-Min Yang, Li Luo, Ling Zhang, Dan-Dan Qi, Song-Xi Shen, Shi-Peng Zhu, Ya-Fang Zhao, Xiao-Xuan Ren, Meng-Wei Guo, Xiao-Hong Li, Bo Ji, Lu-Fen Zhang, and Jiang Zhu. "Effects of Acupuncture Applied to Sanyinjiao with Different Stimuli on Uterine Contraction and Microcirculation in Rats with Dysmenorrhea of Cold Coagulation Syndrome." Evidence-Based Complementary and Alternative Medicine 2014 (2014): 6.
9 Hsu et al., Effects of Acupuncture Applied to Sanyinjiao, pg 6.
10 Hsu et al., Effects of Acupuncture Applied to Sanyinjiao, pg 7.
11 Iacovides, et al., What we know about primary dysmenorrhea today, pgs 765-6.
12 Zahradnik, H. P., and M. Breckwoldt. "Contribution to the pathogenesis of dysmenorrhea." Archives of Gynecology 236, no. 2 (1984): 99-108.
13 Iacovides, et al., What we know about primary dysmenorrhea today, pg 766.
14 Iacovides, et al., What we know about primary dysmenorrhea today, pg 766.
15 Iacovides, et al., What we know about primary dysmenorrhea today, pg 764-5.
16 Armour et al., The role of treatment timing and mode of stimulation, pg 2.